All levels of government, are actively trying to find whatever way possible, to raise tax revenue to fund whatever programs you demand they provide.
Well, of course. To the extent that I and enough other folks demand it, we do need to expect to pay for it. Taxes -- income, payroll and excise -- are the way we do so if the government (state, local or federal) is to administer and deliver the demanded services.
The Federal government also mandated an expansion of Medicaid
The Medicaid expansion was not mandated. Some states adopted it and others did not.
So who is paying for that? You are through state level taxes, or sales taxes, or property taxes.
Yes. I've from the start of this line of conversation agreed that is so. I've also said that I'm okay with doing so to the extent that you cannot afford to pay for your own health care/health insurance. (You recall that is precisely the attestation you made.)
FWIW, I don't get "fussed" about whether I pay the money as property, income or any other tax. My total tax burden matters to me, but as for any specific tax, well, it may irk me if I determine that it is the material cause of my experiencing a "downward" change in the lifestyle I lead. I look at all my expenses/disbursements and consider the total sum I spend in terms of two high level dimensions: discretionary spending and non-discretionary spending. Taxes fall into the non-discretionary segment, except when it's a tax on something I don't have to buy -- for the obvious reason that if the tax I must pay to buy X is so bothersome to me, I just won't buy whatever X is.
Maybe other people don't annually calculate and assess their total tax liability/spending. I don't know. Even as I know about what I pay in taxes, I look at it and form my judgment about it/them based on how it impacts my lifestyle. Truly, my lifestyle is not worse off because of the total sum of taxes I pay.
My awareness of that fact is why, each time you've posted about and shares with increasing levels of detail, I've said that I'm okay with the taxes I must pay that allow you to have health care/health insurance. Perhaps you think I don't know what I pay in taxes, but I do. It all comes down to what my total tax payments are. Thus, unless and until you can give me a credible reason to think my taxes will increase enough to deteriorate the quality of lifestyle I enjoy, my response isn't going to differ. And I write that knowing that in a few years, I'll be fully retired.
As I've intimated already, an increase of ~10% or so isn't going to upset me, particularly if I think it's going, in part, to help relatively poor people who can't afford essential services and goods. On the other hand, an increase of ~25% in my effective total tax rate is almost certain to draw my concern and dissatisfaction. Is there an increase in my total tax rate between 10% and 25% that may also irk me? Perhaps. I can't say just sitting here thinking about it.
Medicare, and Medicaid both, pay less than the cost of care. Obviously no business can stay running if they lose money on most customers. So how do they afford to treat people on Medicare and Medicaid? By charging YOU more. It's simply a tax that doesn't go through the government.
OT:
How providers make profits isn't really part of the scope of what I pay in taxes to subsidize your inability to pay for your health insurance because the fact of the matter is that they currently, as before earn handsome profits. I'm sure they, like everyone, would sooner earn ever more profit. Though Medicare and Medicaid pay less than the "list price" doctors and hospitals quote if one merely asked what be their fee for XYZ procedure,
the program nonetheless pays them sum that allow profitability. Private insurance also pays than the "list price" providers would quote.
So I have no insurance. If I got to the hospital, and they discover I have cancer or something horrendous, I can sign up for Medicaid. You will pay for me through your payroll tax, your federal income tax, your state income tax, your state sales tax, and then through higher premiums because you get charged higher prices to subsidize my medicaid treatment.
Yes. I agree that is what happens.
People believe all sorts of myths about taxes like "My gas tax pays for roads!" Which is exactly what the government wants you to think. In reality those taxes go to the general revenue like all tax revenue does. ]They can "say" that it goes to pay for roads, but in reality once that dollar leaves your hands, it goes where ever they want it to go.
Well, just where it goes and how it's spent depends on the nature of fund into which it goes. If the money goes to the general fund, yes, it can be spent on anything. If it goes to a special fund, it can be used to pay for a limited range of things.
Do you think if the state budget was running a surplus that they would have raised the gas tax? No.
I really can't say what state legislators may or may not do. I know what makes sense and I understand the political realities connected with tax increases, but that doesn't mean they will or won't do what makes sense.
In conclusion, when I say you are going to pay it through higher taxes, I have no idea which tax method the government will use to make you pay for it. But someone has to pay the bill. And the same is true around the world.
Yes, it is.
My experience in looking at various governments is that smaller more regional governments are routinely more effective and less wasteful than larger ones. The government of a city is going to be far more efficient than the government of a massive country.
Hong Kong is an autonomous territory of China; thus it is run as a country as well as as a city.
There was a video of an economist from Sweden, and they were talking to him about the programs the Swedish government has in place, and saying we should do that here. The Swedish economist looked at them like they were nuts and said "Yeah, but the Swedish government is very efficient. Your government is horribly wasteful. If you give them more money, they'll just have more money to waste."
I actually think this is why the founding fathers intended to have a limited federal government, with most of the power left to the states.
I suppose that may be a small part of what they had in mind; however, I'm not convinced it was a key factor. After all, they started the U.S. as a confederation and very soon thereafter learned that wasn't working. Among the most important things the Founders discovered is that balance is preferable to either governance extreme. I suppose that's not shocking as the Founders were uniquely positioned, after the Confederation and having come from a monarchy, to see firsthand the strengths and weakness of a supremely powerful central government as well as those of a supremely weak one. Thus the Constitutional government they created, and the terms of the Constitution itself, came to be as a direct response to the inadequacies of the Confederation of states and to temper the excesses of monarchy.
Beyond that, in looking at the survival rates in Hong Kong, the numbers seem low. Anyone can save money by letting more people die.
Frankly, I'm not convinced that having the highest survival rates (as a nation, not as a doctor or facility) is critical or necessary.
If I opened a hospital, that only used 1990s technology, I can cut the cost of treatment by nearly 50%. The cost of an older Mammogram machine, is only $20,000, compared to a new one that's $500,000. Of course my ability to detect cancer is going to be about 10% lower. Which means survival rates will be lower.
Are you asserting that Hong Kong does not use the latest equipment available? If so, please share some credible documentation supporting the wide applicability in Hong Kong of the scenario you've depicted above. Equally important, perhaps to some more so, whether the latest equipment is used for certain procedures may not necessarily mean that the net quality of care delivered is any worse than that offered using newer, ostensibly more advanced, equipment.
For instance, I have a car from the 1980s and several from 2007 and more recent model years. My old car does not do that which I need a car to do any better or worse than do the newer ones. There are a variety of reasons for that being so; however, the same basic principle -- that at some point "fancier" doesn't, or doesn't materially, improve the outcomes -- is in play as goes the delivery of health care.
One thing I want to note is that you've introduced a discussion about the delivery of health care in Hong Kong. My point for bring up Hong Kong had to do with the system by which that care delivery is paid for and administered, not the care itself. I kept, and want to keep the two separate because one's ability to pay for treatments may well affect what treatments they receive, but it doesn't affect the quality of treatment delivered with regard to the treatments and procedures for which they do pay (or that others will pay for on their behalf).
I know that's a subtle distinction, but it's essential to make it in evaluating pretty much any aspect of a nation's health care system -- both the delivery of the care and how the delivery is compensated. I'm not saying to ignore one or the other, only that they must be compartmentalized, and then considered independently together. (Think of it as being analogous to two line items in a COGS presentation in an income statement.)
Beginning inventory $10,000
+ Purchases 25,000
- Ending inventory 8,000
Cost of goods sold
$27,000
What about
Hong Kong's survival rates dissatisfies you? What survival rate(s) in particular do you mean? Clearly you, in contravention with the analysis of health care experts, you think Hong Kong does not have among the best health care systems in the world.
Hong Kong's health care model seems to be working based on the "full picture" assessments I've seen. Can one hone in one one type of care delivery in that system and take exception with it? Of course. I don't think any nation aims for absolute perfection when tailoring its approach to health care.
The newest and best health care, with the best survival rates, cost premium prices.
As noted above, I don't think that is, in most instances, necessary. I get that a provider may dispose of the old equipment upon obtaining the new. What crosses my mind is that the new equipment isn't always needed.
Take something as simple as a thermometer. The one we can buy in a drugstore measures temperature quite effectively, yet I can't tell you the last time I had a doctor take my temperature with anything other than a newfangled digital thermometer with a disposable plastic covering. Yes, a digital thermometer is a simple and relatively inexpensive piece of equipment, but its prevalence illustrates the point -- just how often is the increase in "whatever" that the new equipment provides necessary -- and that point applies at all levels of treatment delivery. I mean really. Is there anyone working in a doctor's office who can't read a thermometer? If so, those persons should not see patients. Hell, they probably shouldn't even work there if their skills are that limited.
Excess is not limited to equipment purchases/implementations. My father a few years back had to be hospitalized briefly. Instead of sending him home after the hospital was done with him, they wanted him to go to a nursing home, for physical therapy they said, and then discharged from there to his home. For what? The man walked into the hospital and walked while he was in the hospital. They wanted to send him to the nursing home so they couldn't be held accountable if he fell at home after being discharged, and the reason that concerned them is that Dad's in his 90s and walks with a cane. We had to sign a document (I think they called the document an ADA) that effectively waived our right to sue (prevail in any such suit) if he had any misfortunes after being discharged directly home from the hospital. We signed the document and brought him home. He got on just fine.
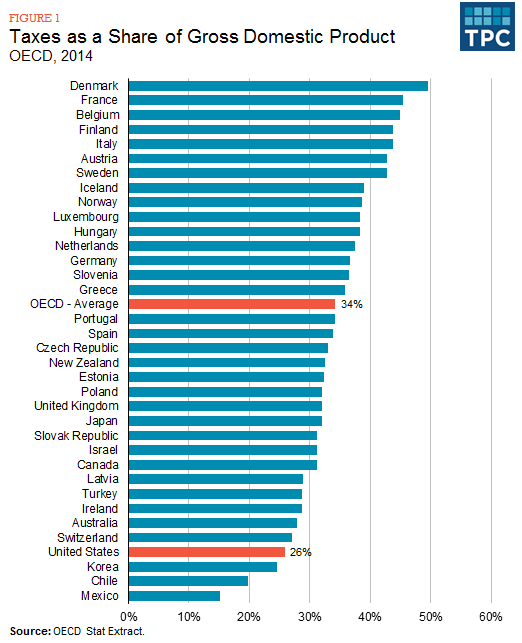
Lastly, your chart again only looked at income tax rates.
Yes. I focused on income tax, federal income tax, because that is the implied nature of the taxes under discussion -- our conversation grew out of remarks pertaining to the ACA.
As I think I successfully showed, income tax is one of many many sources of tax revenue used to pay for health care.
Yes, you have, but I knew so already and would not have differed with you about that being so. As I said, I will stick to the specific scope given by the conversation at the time I enter it. I can't say I never take it upon myself to broaden the scope of a conversation -- I let my reader(s) know I'm doing so if I do so -- but, generally, when I respond to someone, I stick to the scope implicit or explicit in their remarks and the context of the discussion.
")