Your point about seniors carrying auto insurance is not based on an understanding of the difference in economics between young and old, in driving vs. medical expenses.
Young drivers tend to pay more because they have higher accident rates than older drivers, and the risk being insured is much lower (like a $10K-20K auto) so they can still afford the insurance.
When we go to health insurance, those over 65 generally have left the workplace, and they are MUCH worse risks than young people at that age, and the risk being insured is many times higher (like a $100K or $200K hospital stay, nor say $50K annual nursing home expenses).
So, your comparison is invalid economically, the situations are not similar at all. Insuring a car is not the same as insuring a body's health care.
Medicare is the best plan I have seen to provide health care for those over 65. Medicare is not the best it can be, it is too expensive and additional controls and rationing need to be imposed. There is too much fraud in the system, too many start-ups that submit false claims, get reimbursed and shut down before they are caught. They should delay the first payment and always audit the facility before reimbursement begins. Home healthcare businesses provide equipment that is not needed and leave it in homes too long (people ask them to take it out and they don't take it out, saying "well Medicare will pay for it"), and too much is spent in the last year of life and we need better guidelines for that - yes rationing is a valid way to cut costs).
You seem to think Medicare is a fiscally irresponsible way to provide healthcare to those over 65 without offering an economically valid alternative.
I think Medicare is a valid structure, the best I've seen, to provide healthcare to those over 65, and it has some problems and it needs to become more efficient.
"...without offering an economically valid alternative. "
Get out your pencil and paper, Beady, as I'm about to blow your status-quo five-minutes-ago thinking out of the water!
The basis of your post is totally hypothetical...so let me have a go at it:
Free-Market, Beady....
1. Open the market, competition will drive down the costs: more companies will offer the insurance due to more customers and less gov red tape.
2. Reform of Insurance Policy Mandates:
Scrap all city, state, federal mandates for healthcare insurance policies. When a statute says policies must cover mammograms of everyone 35 and over, how is this fair for a construction company with all male employees? What about Podiatry, or sexual reorientation surgery/? Allow insurance companies to write policies covering exactly what the consumer asks for:
Take two very different states: Wisconsin and New York. In Wisconsin, a family can buy a health-insurance plan for as little as $3,000 a year. The price for a basic family plan in the Empire State: $12,000. The stark difference has nothing to do with each states health sector as a share of its economy (14.8 percent in Wisconsin as of 2004, the most recent year for which data are available, and 13.9 percent in New York). Rather, the difference has to do with how each states insurance pools are regulated. In New York State, politicians have tried to run the health-insurance system from Albany, forcing insurers to deliver complex Cadillac plans to every subscriber for political reasons, driving up costs. Wisconsins insurers are far freer to sell plans at prices consumers want.
The gulf in insurance-premium prices among American states is a sign that too much government interventionnot too littleis whats distorting prices from one market to the next. The key to reducing health-care costs for patients, then, is to promote competition, not to dictate insurance requirements from on high. Unfortunately, a government-run insurance plan is the core of ObamaCare.
Bigger Is Healthier by David Gratzer, City Journal 22 July 2009
a. NJ has some 68-69 mandates including
in vitro fertilization, which adds some 2-2.5% to the cost of the policy
3.. Doctors currently have no ability to
re-price or re-package their services that way every other professional does. Medicare dictates what it pays for and what it wont pay for, and the final price. Because of this there are no
telephone consultations paid for, and the same for e-mails, normal in every other profession.
Most doctors dont
digitize records, thus they cannot use software that allows electronic prescription, and make it easier to detect drug interactions or dosage mistakes. Again, Medicare doesnt pay for it.
4. Another free market idea aimed at better quality is have warranties for surgery as we
do for cars. 17% of Medicare patients who enter a hospital re-enter within 30 days because of a problem connected to the original surgery. The result is that a hospital makes money on its mistakes!
5.
Walk-in clinics are growing around the country, where a registered nurse sits at a computer, the patient describes symptoms, the nurse types it in and follows a
computerized protocol, the nurse can prescribe electronically, and the patient sees the price in advance
6. To reduce healthcare costs,
increase the number of doctors. Obama care would do the opposite. Both tax incentives and support of the tuition of medical school.
7. Identify the 8-10 million who need and are
unable to get healthcare, including those with pre-existing conditions,and provide debit cards as is done for food stamps:
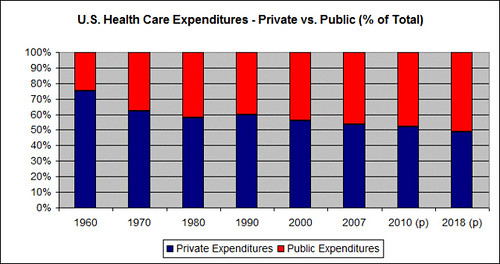
"Food debit cards help 27 million people buy food, similar to the number who need help buying health coverage. In all fifty states, debit card technology has transformed the federal food stamp program, which used to be notorious for fraud and abuse. (Only 2 percent of card users are found to be ineligible, according to the General Accounting Office.) Cards are loaded with a specific dollar amount monthly, depending on family size and income, and allow cardholders to shop anywhere. The same strategy could be adapted to provide purchasing power to families who need help buying high-deductible health coverage. It's what all Americans used to buy (see chart 5), and it's all that's needed for families with moderate incomes, who can afford a routine doctor visit. "
Downgrading Health Care
8. Current law provides unlimited
tax relief for coverage obtained through an employer but no comparable relief for those who purchase coverage outside their places of work. S. 334 would replace the current tax preference for employer-based health coverage with a new individual-based system. The bill would
end the tax exclusion in the personal income tax for employer-based health insurance benefits and instead use a combination of subsidies and tax deductions for health insurance. Ideally, the current employer-based tax structure should be replaced with a fair and equitable universal tax credit. An across-the-board, fixed-dollar health care tax credit, for example, would offer every American federal tax relief for health care.(Wyden-Bennett Bill)
PoliticalChic said:
1. Open the market, competition will drive down the costs: more companies will offer the insurance due to more customers and less gov red tape.
This is not true. The US spends 17% of GDP on healthcare, while Canada and England and most European nations with national healthcare spend 10%. Healthcare costs are and have been increasing at twice the inflation rate for decades, which is why more and more businesses were dropping health insurance coverage. And all this is while insurance companies and their current death panels can drop coverage to customers who get too sick or deny coverage to people with pre-existing conditions even if they previously had coverage for years and lost it due to losing a job.
You have not stated what a health insurance premium for a 70 or 80 year old person would be, if we did not have medicare. I looked up for Texas, for a 64 year old person (that is the oldest quote available, after that they assume you will be on medicare), and it is about $500 per month for a $5,000 deductible policy. You can assume that is for a healthy 64 year old without a pre-existing condition, as we know private health insurance companies reject those folks. So, what would it cost to insure a 70 year old, and 80 year old, a 90 year old, a 100 year old, and a 110 year old (yes, some people live that long, and a national health care system needs to plan to cover them also, unless we want to just let our very old die outside). Should the private insurers you envision be allowed to deny coverage to 90 year olds with pre-existing conditions like cancer? What would that monthly policy cost? How many people could afford that type of coverage? Has anyone seen an actual proposal of this type, that spells out how it would actually work? I have not, and it does not seem economically feasible to me. The monthly cost to retirees would be too expensive for the vast majority to afford IMO.
This is a really, really weak post. Americans have the greatest life expectancy...the WHO stats are a fraud, the vast majority of folks were perfectly happy with their healthcare before Obamacare,
Vague, all over the map, and asking me to provide a price for a premium....but you write, "you can assume," "I have not" seen data....
pretty bogus.
why are you so afraid of a free market approach?
So here's more so you can have nightmares:
1. Government actually subsidizes healthcare for the wealthy. Pennsylvania ran a commercial stating No family makes too much money for low-cost CHIP (Childrens Health Insurance Program), so apply today. Dont think you make too little or too much.
CHIP Error
2. The group that is chronically uninsured, and does not include illegal aliens, those making over $75,000, are not currently eligible for government programs, is in the area of 3% of the population.
http://www.coverageforall.org/pdf/BC-BS_Uninsured-America.pdf
3. Blue Cross/Blue Shield, Aetna, Humana, and many other insurers offer basic youth-oriented health-insurance plans for around $50 a month, depending on homestate (since we cant buy insurance across state lines).
Health Insurers Target The Individual Market - WSJ.com
So, which is higher, the healthcare or cell phone plan?
When you give free insurance to someone who can afford it, but who chooses to spend their money on other things, you are in effect paying for those other things.
4. Can you force those who choose not to be insured to get health insurance?
Even in good times, many Americans drive without insurance. The Insurance Research Council's previous study, released in 2006, found that nearly 15% of drivers nationally were uninsured in 2004, up from about 13% in 1999. In some states, including Mississippi, California and Arizona, roughly a quarter of drivers weren't insured.
And this is even though auto insurance is required in 48 states, costs less than health insurance, and jail time is possible!
Road Risks Rise as More Drivers Drop Insurance - WSJ.com
5. Universal Healthcare Around the World:
Italy: average wait for a mammogram is 70 days
When you compare the outcomes for specific
diseases, the United States clearly outperforms
the rest of the world. Whether the disease
is cancer, pneumonia, heart disease, or
AIDS, the chances of a patient surviving are far
higher in the United States than in other countries.
The same is true for prescription drugs.
For example, 44 percent of Americans who
could benefit from statins, lipid-lowering
medication that reduces cholesterol and protects
against heart disease, take the drug.
That number seems low until compared with
the 26 percent of Germans, 23 percent of
Britons, and 17 percent of Italians who could
both benefit from the drug and receive it.
http://www.cato.org/pubs/pas/pa-613.pdf
In Great Britain, about 20% of patients with treatable colon cancer at the time of discovery are considered incurable by the time treatment is finally available.
http://www.cato.org/pubs/pas/pa-613.pdf
Countries in which complementary or supplementary private health insurance policies are common include
Belgium, Canada, Denmark, France, Germany, the Netherlands, New Zealand, and the United States (in
the case of Medicare programme beneficiaries).
In countries where private health insurance is available, governments often impose rules on what sort of
coverage is permissible. For example, Australia prohibits private insurance policies from covering the
ambulatory care co-payments required in the public programme. Canada prohibits private health insurers
from covering benefits included in the national plan.
The public-integrated model combines on-budget financing of health-care provision with hospital
providers that are part of the government sector.6 These systems, which merge the insurance and provision
functions, are organised and operated like any government department. Staff is generally paid on salary
(although, in some cases, doctors can have private patients as well) and they are most often public-sector
employees. Ambulatory doctors and other health-care professionals can be either public employees or
private contractors to the health-care authority, with a range of remuneration packages. Ensuring complete
population coverage is particularly easy under such systems, and as they are under the control of the
budget, the growth of overall costs has been contained more easily. However, they have weak incentives to
increase output, improve efficiency, or maintain quality and responsiveness to patient needs.
6. National Institute for Health and Clinical Excellence (NICE): tells Brits if their life is worth living- in actual dollars and cents. As the NYTimes states, its job is to develop a standard method of rationing. NICE has decided that Britain, except in rare cases, can afford only £15,000, or about $22,750, to save six months of a citizens life.
(
http://www.nytimes.com/2008/12/03/health/03nice.html)
So, the average one-bedroom apartment in Manhattan is worth way more than a Brits life!(
March 2009 Manhattan Rental Market Report | Rental Market Reports | TREGNY)
So, it has concluded that if you have breast cancer, the drug Tykerb, shown to delay the progression of the disease, is worth more than you are despite Glaxos offer to pay for the first 12 weeks of treatment.
U.K. Says Tykerb Isnt Worth Cost, Even With 12 Free Weeks - Health Blog - WSJ
The Bush Administration sent chief medical officer of the Center for Medicare and Medicaid Services, Dr. Sean Tunis to learn about NICE and try to adopt the processes and mechanisms they used, and we just couldnt
[use]price to determine which drugs or devices Medicare or Medicaid provides has provoked fierce protests.
http://www.nytimes.com/2008/12/03/health/03nice.html
7. WHO/UN
So we have been told that the United States is listed at number 37 in world ranking for health care.
Here is why only fools and America-bashers attribute any significance to this rating: WHO/UN states that their data is hampered by the weakness of routine information systems and insufficient attention to research and when they couldnt find data, they developed [data] through a variety of techniques. WHO accepts whatever governments tell them, including reputable regimes such as Castros Cuba.
WHO | Message from the Director-General
8. Now, who are you going to believe if not Michael Moore? Moore states that Cuba has a better healthcare system (they live longer). "All the independent health organizations in the world, and even our own CIA, believes that the Cubans have a pretty good health system. And they do, in fact, live longer than we do," he said.
But when "20/20" contacted the CIA, officials said, "We don't say that Cuba has a pretty good system or that Cubans live longer than Americans."
In fact, the CIA's World Fact Book says Americans live nearly a year longer. Although a U.N. report supports Moore's position, that data comes straight from the Cuban government.
Healthy in Cuba, Sick in America? - ABC News
9. If you think healthcare is expensive now, wait until its free:
The following Universal Healthcare countries have higher out-of-pocket costs than the United States:
Out-of-pocket spending as a share of total expenditure on health, 1980-2000
http://www.oecd.org/dataoecd/5/53/22364122.pdf (table 4)
Canada, Denmark, Finland, Italy, Spain, Switzerland.
10. How to judge healthcare:
a) life expectancy: many people die for reasons that cant be controlled the medical profession, such as auto accidents, murder, etc., and once you factor out care crashes and homicides, the US ranks number one in worldwide life expectancy!
One often-heard argument, voiced by the New York Times' Paul Krugman and others, is that America lags behind other countries in crude health outcomes. But such outcomes reflect a mosaic of factors, such as diet, lifestyle, drug use and cultural values. It pains me as a doctor to say this, but health care is just one factor in health.
In The Business of Health, Robert Ohsfeldt and John Schneider factor out intentional and unintentional injuries from life-expectancy statistics and find that
Americans who don't die in car crashes or homicides outlive people in any other Western country.
And if we measure a health care system by how well it serves its sick citizens, American medicine excels.
Dave Petno | On Freedom
11. Free-Market Innovations
a) Walgreens has retail health clinics staffed by board-certified Family Nurse Practitioners and Physicians Assistants, and expects to have 400 open by 2010, and CVS plans on about 500. Anyone can walk in and get treatment for about 1/6 the cost of an emergency room, plus about 2/3 are paid for by insurance. Treatment includes: Respiratory Illnesses
Additional Treatments
Skin Conditions
Minor Injuries
Diagnostic Testing
Wellness
Vaccinations
About Us - Take Care Clinic - Convenient, Affordable Health Care
b) Wal-Mart offers some 400 different prescription drugs @ $10 for a 90 day supply. CVS, Target, Kroegers, Food Lion, and a number of others have similar plans.
c) eHealthinsurance.com allows you to find health insurance in your zip.
d) Healthcarebluebook.com tells the costs of various procedures and treatments, allowing the consumer to negotiate prices with practitioners.
e) Teledoc gets you on the phone with a licensed physician in 3 hours or less, for $35- or its free!
f) American Well will let you talk to a doctor by webcam, text, phone, or IM for $45. And some Wal-Marts have virtual clinics where they can actually look into eyes, ears, and throat by webcam.
American Well - FAQs
g) For an annual fee of just $480 for singles ($580 for couples and $680 for families) The No Insurance Club offers affordable pre-paid health care plans that cover basic medical services from a participating board-certified physician, with no deductibles, no additional premiums, and no co-payments and either 12 or 16 visits per year.
NoInsuranceClub
h)
Cosmetic surgery is the closest thing we have to a true free-market system in American. No insurance coverage, and the consumer shops around among practitioners: the price has been falling over time in real terms despite a huge increase in volume and considerable technical innovation (which is blamed for increasing costs for every other type of surgery).
In summary, as far as your defense "This is not true."
I counter with "Is too."