Moonglow
Diamond Member
If that is true you would be on SSDI. Fail, try again.
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.

Clinics outside the capital have been complaining of drug shortages, especially of HIV test kits and ARVs. John Barasa, who heads an ARV clinic in Busia in eastern Uganda, says the government is not been delivering all of the drugs his facility orders. Of the 100 packs of ARVs the clinic requested in June, he says, only six were delivered. To make up for the shortages, Barasa has been stretching his supplies by giving patients only one or two weeks worth of drugs at a time. "Some, who have to travel for hours to reach the clinic, have been running out of medicine," he says.
Elvis Basudde, head of the Positive Mens Union, says he has been receiving complaints of drug shortages from clinics across the country. For HIV-positive Ugandans, he says, lack of access to ARVs could be disastrous. "With us, there must be strict adherence to treatment," Basudde said. "So whenever we have such problems and issues, and somebody cannot be able to access medicine in good time, you can imagine the consequences. It could lead to drug resistance." Yet Ugandan health advocates such as Margaret Happy, who works with the National Forum of People Living with HIV, say that there is no shortage of drugs in the country. "At facility level, it is very severe," she said. "However, at national level the situation seems to be very different."
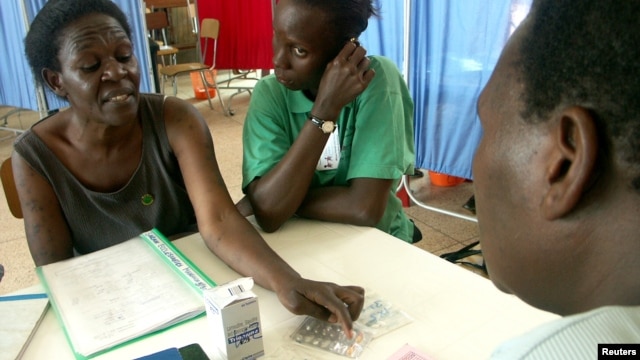
Ugandan HIV/AIDS patients listen as a Mbuya Community Outreach doctor explains how to start anti-retroviral treatment, near Kampala
According to the Ministry of Health, Uganda has plenty of ARVs, enough to last until December. Ministry spokesperson Rukia Nakamatte says the problem lies with the clinics themselves, and with health workers who do not know how to use the governments new Internet-based system for ordering medicine. "The current shortage that we are experiencing in some facilities is due to increased orders that are being placed wrongly," Nakamatte said. "We have problems with some data entrants and bio-statisticians who are not able to enter the right data."
But in the clinics visited by Happy, this hasn't been the case. "National level transfers blame to the local level. Yet the local level [has] evidence that clearly shows that they make the right quantification, and they make it timely," she said. "The problem is with delivery." Happy says the new web-based order form is not always functional, and some of her fellow advocates also blame a new national supply system that prevents facilities from boosting each others supplies. Both systems would be good ones if they worked, Happy said, adding that unless Ugandas ARVs can make it out of the warehouses and into the clinics, they will not be saving anyone.
Uganda Health Clinics Face AIDS Drug Shortages
This is the second time this year that the more than 500,000 people living with HIV in Zambia have had to cope with what the Ministry of Health calls rationing of the drugs - a system that some patients here have been contending with for more than a decade. It is a bitter pill to swallow, especially because obtaining medicine is not as easy as one would think. A check at some clinics in Lusaka shows that patients must turn up at 4 a.m. to queue services they will only receive hours later. Zambias Ministry of Health admits there is a challenge regarding the stocks of ARVs in the country, which it refers to not as a shortage, but as "rationing."
Chikuta Mbewe is the deputy director of pharmaceutical services. He said part of the problem was an ongoing switch in Zambia and other countries from one drug, Truvada, to another, Atripla. Mbewe said complications with the switch have driven down the stocks of both drugs. "I must hasten to say that there are a lot of planned shipments that have already started arriving in the country. We think now we are in the normalization curve, so to say. We hope we can get back to our normal levels, he said. Mbewe said the Zambia government wanted as many people as possible to be on [taking] Atripla, since an eight-month supply of the drug was expected to arrive in Zambia before the end of October. Mbewe said the governments strategy was to get 95 percent of people living with HIV using Atripla, to simplify the supply chain.

An HIV-AIDS patient (R) places her hand on her forehead during a visit by a caregiver at her home in Matero township on the outskirts of Lusaka, Zambia
But Felix Mwanza, national director of the Treatment Advocacy and Literacy Campaign, believed the ARV situation in Zambia could have been avoided with proper planning. To us, when they say the situation will improve by October, I think justifies what we have been saying," said Mwanza. "I think there is more than what the naked eye actually sees. Because if the government were saying initially that it will take two weeks for the situation to improve, and they and they move on to say that it will improve in one month's time - and this time they are talking about October - then who is telling the truth? So people should actually be asking questions, [such as] 'Is there something amiss?'"
Whatever the cause, the shortage is real. Ackim Sakala, a primary school teacher who has been living with HIV for 12 years, is not happy that he has to go to the clinic every month to collect his ARVs, though he acknowledged the situation could be worse. His clinic is only a kilometer away. I can imagine for those that walk long distances, I know what they are passing through. From the experience that I have had some people have been rationed to two weeks and you can imagine every two weeks they have to get to the clinic to collect their drugs. For sure there is a shortage," he said.
One of the long-term interventions that Zambias Ministry of Health wants to achieve is to attract investors to set up a pharmaceutical plant that will not only manufacture ARVs in the country but other essential drugs as well. In the meantime, all the people living with HIV have to face the grim reality of what the authorities are referring to as rationing, when the people that use the drugs call it a shortage.
Source
Stop sending aid to africa. Let africa die.
It's more inhumane to keep a dieing corpse alive than letting the corpse just die and end its misery.
Stop sending aid to africa. Let africa die.
It's more inhumane to keep a dieing corpse alive than letting the corpse just die and end its misery.
I bet you consider yourself a Christian. You sickening fuck.
Stop sending aid to africa. Let africa die.
It's more inhumane to keep a dieing corpse alive than letting the corpse just die and end its misery.
I bet you consider yourself a Christian. You sickening fuck.
Stop sending aid to africa. Let africa die.
It's more inhumane to keep a dieing corpse alive than letting the corpse just die and end its misery.
I bet you consider yourself a Christian. You sickening fuck.
110% Atheist.
I bet you support aid to africa don't you?
Feeding a starving african so they can turn around and starve some more is more inhumane than letting that african die. You twisted degenerate.
I bet you consider yourself a Christian. You sickening fuck.
110% Atheist.
I bet you support aid to africa don't you?
Feeding a starving african so they can turn around and starve some more is more inhumane than letting that african die. You twisted degenerate.
So you would prefer to wipe out millions of people just because they are poor?
Sick freak you are.
Sigh.
This forum sucks. There's too many idiots here.
And TAXPAYERS ON HOOK? That about it twerp?If that is true you would be on SSDI. Fail, try again.
Black Gay Teen Prostitute Robert Rayford was the first known aids case in the USA in early 1968 St. Louis, MO. Thank him & his sex partners for the US aids epidemic.