You know, it doesn't take long to discredit that which has not been proven to be a final product. Among this group, 25 patients are now cured and 16 are still hospitalized (98% of patients cured so far). Poor clinical outcome was significantly associated to older age (OR 1.11), initial higher severity (OR 10.05) and low Do they know the exact age cut off? How are the 16 who are still hospitalized? Do you know? Do we know? No! Keep at it. And remember one thing, while your promoting your new found drug, most young patients recover without any treatment. Doesn't appear the drug does to well with old patients though. Keep trying.
Hah.
Sure.
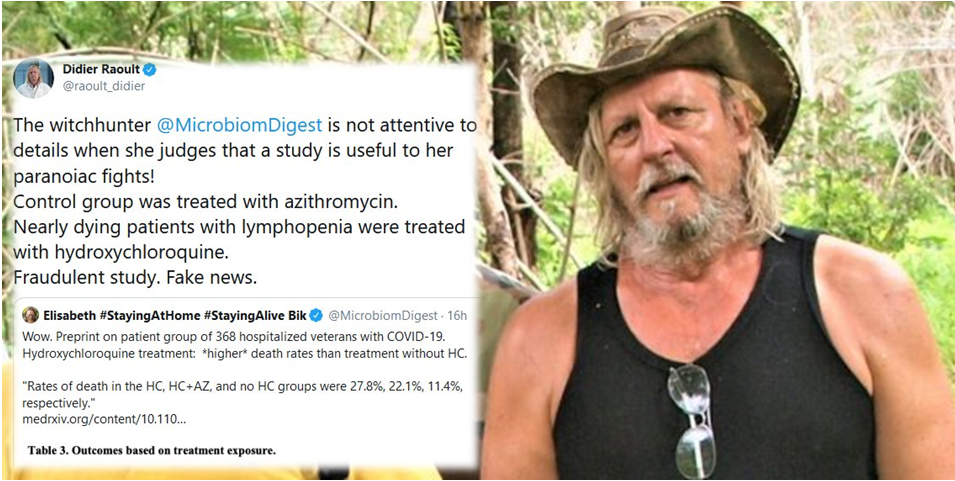
Coming from someone who demands absolute perfection from studies he apparently doesn't read through.
"Huang et al. reported the clinical features and cytokine profile of critically ill patients with COVID-19 in Wuhan, China, and suggested that a cytokine storm (i.e. higher concentrations of granulocyte-colony stimulating factor, interferon gamma-induced protein 10, monocyte chemoattractant protein 1, macrophage inflammatory protein 1α and tumour necrosis factor α) could be associated with the severity of disease."
Recently, chloroquine and its derivative hydroxychloroquine have been used in the treatment of COVID-19. In February 2020, results from more than 100 Chinese patients with COVID-19 showed that chloroquine phosphate had good efficacy
[8]. French doctors conducted an open-label non-randomized clinical trial, and 20 patients with COVID-19 who received hydroxychloroquine treatment showed good efficacy
[9]. Both chloroquine and hydroxychloroquine are weak bases and are able to accumulate in acidic organelles (e.g. lysosomes); as such, they can increase endosomal/lysosomal pH and inhibit viral replication
[10]. In addition to their antimalarial and antiviral effects, their anti-inflammatory properties have been demonstrated in the treatment of autoimmune diseases such as rheumatoid arthritis and lupus erythematosus. Chloroquine and hydroxychloroquine can inhibit major histocompatibility complex class II expression, antigen presentation and immune activation (reducing CD154 expression by T cells) via Toll-like receptor signalling and cGAS stimulation of interferon genes
[11]. Thus, chloroquine and hydroxychloroquine can reduce the production of various pro-inflammatory cytokines, such as IL-1, IL-6, interferon-α and tumour necrosis factor, which are involved in the cytokine storm
[11]. These immunomodulatory effects synergize their antiviral effects in the treatment of COVID-19.
Immunomodulatory agents that directly target the key cytokines involved in COVID-19 may also help to alleviate hyperinflammation symptoms in severe cases
[12]. Elevated levels of the inflammatory indicator IL-6 in the blood have been reported to be predictive of a fatal outcome in patients with COVID-19
[13]. Tocilizumab, a specific monoclonal antibody that blocks IL-6, has been recommended for use in severe or critically ill patients with extensive lesions in bilateral lungs and a confirmed elevated level of IL-6 in the Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7) issued by the National Health Commission of China
[7]. A retrospective analysis on 20 severe cases of COVID-10 showed that treatment with tocilizumab led to a reduction in fever and lung lesion opacity, and recovered the percentage of lymphocytes in peripheral blood
[14].
Discussion of the role of immunomodulatory agents to reduce the cytokine storm in severe cases of COVID-19. Potential immunomodulatory agents currently used in the treatment of COVID-19 (chloroquine, hydroxychloroquine and tocilizumab) are ...

www.ncbi.nlm.nih.gov