In any other market, without government intervention, a transparent market organically evolves into being.
Neither health insurance nor health care are office supplies. I thought that comparison above was in jest but now I'm beginning to think you're serious. The market structure and the incentives in question are unique and rather complex. That's why health economics exists as a sub-discipline. Health care is not and will never be "any other market," which is why we're even talking about it.
That pretty much covers every single bed in the entire hospital, that a patient spends a night in.
We'll no, it doesn't. "Skilled nursing" is not simply another name for "nursing," it pertains to a specific type of custodial care offered in a long term care facility (namely a SNF or other LTC setting). It doesn't apply to standard acute care settings. Ohio appears to have no CON requirements for acute care settings or emergency care.
Like I said, you need to find a different explanation.
And yes, I get that hospitals love the CON laws
, so that they won't go out of business.
Hospitals
are going out of business, even (perhaps especially) in areas where they have no competitors. As I already mentioned, inpatient occupancy, and thus revenue, has been in a state of decline.
For example, why does it cost so much to get aspirin in the hospital? One reason is, according to Federal law, they can't buy a bulk container of aspirin, but rather individually wrapped aspirin. And they can't just have an nurse in training, or intern, give you the aspirin. No it must be a Registered Nurse or LPN, which of course costs a ton of money, to pay someone $70,000 to hand out Aspirin.
Hospital charges have very little to do with what anything actually
costs. They mark up virtually everything because (1) they can, and (2) they're cross-subsidizing other services or expenses on which they would otherwise lose money.
You say "hospitals have high fixed costs" as if that's a given. No, it's not. They have high fixed costs, because government requires them to.
Hospitals are expensive organizations. They're generally prepared for a huge variety of eventualities and they tend to be the largest nongovernmental employer in a region.What cost is it you propose to eliminate through the magic of regulation? Staff salaries?
All of the competition in the world in the insurance market, won't lower costs by very much. The poison of spiraling costs of health care, goes all the way down to the roots of the constraints of medical schools training limited numbers of doctors, all the way up to the top of individuals buying insurance.
The exchanges have already shown very clearly that insurers competing in a real market on premium (which, granted, is a pretty new phenomenon for them) will either negotiate down prices with providers or exclude high priced providers from certain networks entirely. They'll support alternative payment models meant to support cost-saving, efficiency-promoting reorganizations of care delivery. And they'll devise insurance products meant to both encourage health on the part of consumers and make them more price sensitive when they actually look to access health care services. And that's why their premiums have been surprisingly low.
You *seemed* to imply that Obama Care leads to a structured market, and that we would want to move people off of Employer Sponsored Insurance, into this structured market.
The ACA has created a structured
individual market, and price competition had been extremely robust (lower-than-projected premiums are one of the reasons the law is coming in hundreds of billions under budget.)
The group markets still exist and indeed the law has an employer mandate to preserve the status quo. But small (and ultimately large) employers can make use of the exchange infrastructure. And I have little doubt that exchanges will be the way forward for any market based approach to health insurance.
I am absolutely serious. You can say "Health care isn't like office supplies" and yet what we have seen here in America, and around the world, is the fundamentals of economics work exactly the same. You can say it's not the same, but it works the same. You limit entry into the market... price goes up. You regulate the market.... price goes up. You limit competition in the market... price goes up. You attempt to control the price... shortages show up.
This is why you have places like India, where medical tourist hospitals, that are free from the regulations of the government, and are only controlled by the chaos and wild-cat fundamentals of economics based on supply and demand.... and you can have a surgery that cost $100,000 in the US, cost only $18,000 in India.
The fundamentals of economics don't magically change, because "this is health care!".
And every time you do, the result is disaster. Energy isn't like office supplies.... right? And then you end up with rolling black outs across California.
CON laws
But I posted the specific law, which said "Skilled Nursing, or Nursing.". Nursing or skilled nursing. That pretty much covers all nursing of any kind. Name a bed in a hospital in which there is no nurse in attendance?
You can't, and I can tell you why. I posted the list of laws governing hospitals, and one of the requirements is that there is a nurse assigned to every single bed which has a patient. By law, every single bed, has a nurse.
Now maybe there is some other part of the law, that I don't know about..... but.... based on what I read, CON laws cover every single bed in any hospital in the state of Ohio.
Hospitals are going out of business, and hospitals mark up everything they can, because they can and to subsidize other services they would lose money on.
Most of what you said is true, with the exception of "because they can". Clearly if hospitals are closing..... then they are marking up prices because they are trying not to close.
But what all of what you said, ignores the cause. Here is the cause....
Analysis: Why Rural Hospitals Are Closing | Daily Yonder | Keep It Rural
I have to admit I love these small time media outlets, who are not driven by a political bent, and have no problem just saying the truth.
In 1984 Congress changed the way Medicare paid hospitals. Instead of paying whatever hospitals claimed for taking care of Medicare patients, the agency began paying what it judged was reasonable for a particular illness.
That change was hard on a lot of hospitals, but the larger ones were able to live with it. For bigger hospitals, the length of patient stays averaged out. And, to the extent that Medicare was systematically underpaying, hospitals raised their charges to private insurance companies to make up the difference.
So Congress decided to determine how much is reasonable to pay, instead of hospitals telling government how much it cost them to provide care. Why? Because Medicare expenses were growing at an unsustainable rate.
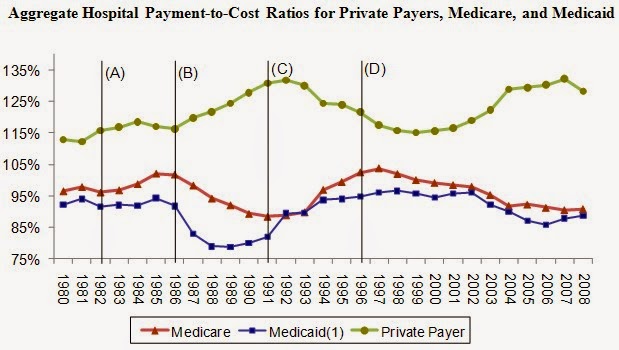
Medicare under pays hospitals. So larger hospitals increase prices on privately insurance patients, to subsidize the cost of Gov-Patients on Medicare and Medicaid.
Small rural hospitals don't have that as an option, because most of the people in rural towns are on Medicare. The younger people generally move into the city to find work.
Now as you can see, every time that Medicare and Medicaid pay out less and less for care, the hospitals cost-shift that to private patients in higher and higher mark ups.
And what you just pointed out, was that they are not doing it because "they can", they are doing it because if they don't.... like rural hospitals can't... then they close.
The story goes on.......
In 1997 Congress authorized the Critical Access Hospital system to help fix these problems. The new bargain was, if a hospital of up to 25 beds in a rural area would accept some limitations on how long a patient could stay (a practical way to require them to transfer complicated cases), Medicare would pay them what the hospital reported it cost to take care of Medicare patients.
When Congress drafted the Affordable Care Act, it scheduled phase out of most of those special payment programs.
Have you ever wondered why you go to an inner city hospital, and find people there from an hour away? I've worked in hospitals, and that always confused me. This is why. The smaller hospitals were transferring patients out of their hospital, to bigger hospitals that could cost-shift the lack of payment from Medicare.
But Obama Care has started phasing out those programs. Why? Again, it's too expensive. They had to make Obama Care seem as though it wouldn't break the Federal Budget. So they cut some of these programs, that kept those rural hospitals alive.
All of this is to point out the regulation, and government intervention, is what has caused all of this. If every single patient, paid for their own care, we wouldn't be talking about this. Hospitals wouldn't be cost-shifting to private patients, jacking up prices. Rural hospitals would be charging what it cost to provide care, and not be closing. No one would be transferred hours away from friends and family.
What cost do I propose to eliminate through the elimination of regulation?
Well... everything I just listed above, for starters. I think we can hire interns and trainees to hand out cups of water and aspirin, instead of a $80,000 Registered Nurse. How about eliminating all the controls on Medical Schools? Supply of doctors goes up, cost of doctors goes down. Simple economics.
If it didn't cost $300,000, and take 10 years, to go through medical school, I wager doctors would be willing to work for less.
And honestly, we don't know what all could be done to lower cost, because no one can do anything to lower cost under the current system.
But you can't tell me that reducing or eliminating regulation can't possibly result in lower cost, because we can look around the world, and see that hospitals that do not have the regulations we do, operate at a fraction of our cost.
Who knows what new method of health care could be developed in a system where they are not constrained by government controls?
The exchanges have already shown very clearly that insurers competing in a real market on premium (which, granted, is a pretty new phenomenon for them) will either negotiate down prices with providers or exclude high priced providers from certain networks entirely.
They were doing that before the exchanges existed. That's actually part of the problem. Hospitals increase prices, to account for the negotiated discount. If a treatment costs $1,000, and the insurance companies have a 50% discount, how much does the hospital charge? $2,000.
This system harms the uninsured the most, because they have to pay the full, made up, price.
This is one of the reasons we don't have a transparent market. All of those costs on those bills are made up numbers, to account for the cost-shifting regulations, and the negotiated discounts. Again, if we had zero regulations..... all of that would go away.
The ACA has created a structured individual market, and price competition had been extremely robust (lower-than-projected premiums are one of the reasons the law is coming in hundreds of billions under budget.)
How do you claim, a market that has shrunk in size, is 'robust'? I just posted the raw numbers. The individual market has declined.
And no, the reason the law has come in under the budget, is because very few of the uninsured, got insurance. The budget was based on the idea that all 45 Million of the uninsured, would get insurance. That hasn't happened.
And I don't think price competition has been so great. The only reason prices have no gone up... is because benefits have declined. The base deductibles have increased dramatically.
Pretty easy to hold prices down, when you cut benefits by a ton.