
- Jan 23, 2021
- 6,307
- 7,140
- 1,938
The state of health science today is such that the loudest opinion wins.
Follow along with the video below to see how to install our site as a web app on your home screen.

Note: This feature currently requires accessing the site using the built-in Safari browser.
Certainly there is a conservative press in America that is covering the fallout from these shots??? Or are you being a conspiracy theorist now?Because for now the American press won't cover the fallout from these shots.
However at this rate this won't last much longer. It can't be kept quiet for much longer at all. The only thing that has kept it muted til now is the deluge of other bad news: inflation, gas prices, Ukraine. Hard to know if that's on purpose. But even so. All these 20s/30s people having heart attacks?? Not much longer.
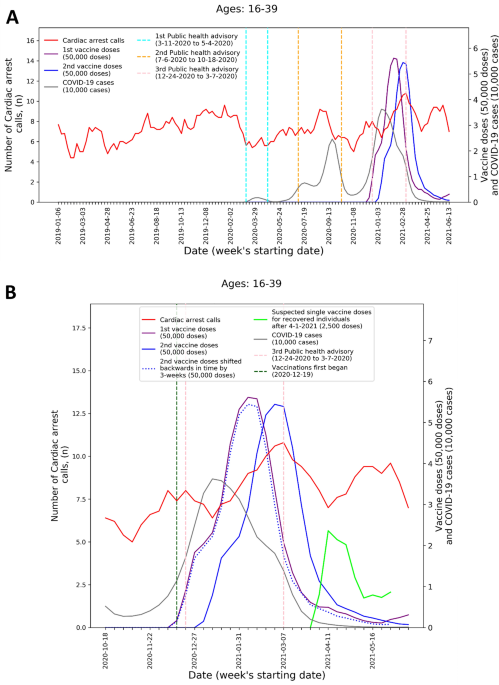
Moreover, it underscores the need for the thorough investigation of the apparent association between COVID-19 vaccine administration and adverse cardiovascular outcomes among young adults. Israel and other countries should immediately collect the data necessary to determine whether such association indeed exists, including thorough investigation of individual CA and ACS cases in young adults, and their potential connection to the vaccine or other factors. This would be critical to better understanding the risk-benefits of the vaccine and to inform related public policy and prevent potentially avoidable patient harm. In the interim, it is vital that following vaccination, patients should be instructed to seek appropriate emergency care if they are experiencing symptoms potentially associated with myocarditis, such as chest discomfort and shortness of breath, as well as consider avoiding strenuous physical activity following the vaccination that may induce severe adverse cardiac events.
 www.nature.com
www.nature.com
1.The studies coming out about the efficacy of the mRNA vaccines is stunning.
the term often forwarded is 'monoclonal antibodies' ....Once the active antibodies are gone from a mRNA virus you are again at risk to become ill. Without the formation of long term immunities in your bone marrow which look for the virus you do not gain these.

file:///C:/Users/family/Downloads/jamacardiology_montgomery_2021_br_210004_1633734807.98598.pdf1.
European Medicines Agency (EMA). COVID-19 mRNA vaccines Comirnaty and Spikevax: risk of myocarditis pericarditis. Published online July 19, 2021. Accessed November 9, 2021. COVID-19 mRNA Vaccines Comirnaty and Spikevax: risk of myocarditis pericarditis - European Medicines Agency
2.
Mevorach D, Anis E, Cedar N, et al. Myocarditis after BNT162b2 mRNA vaccine against Covid-19 in Israel. N Engl J Med. Published online October 6, 2021. doi:10.1056/NEJMoa2109730
3.
Witberg G, Barda N, Hoss S, et al. Myocarditis after Covid-19 vaccination in a large health care organization. N Engl J Med. Published online October 6, 2021. doi:10.1056/NEJMoa2110737
4.
Klein NP, Lewis N, Goddard K, et al. Surveillance for adverse events after COVID-19 mRNA vaccination. JAMA. 2021;326(14):1390-1399. doi:10.1001/jama.2021.15072
ArticlePubMedGoogle ScholarCrossref
5.
Centers for Disease Control and Prevention Advisory Committee on Immunization Practices meeting. Myocarditis analyses in the vaccine safety datalink: rapid cycle analyses and “head-to-head” product comparisons. October 21, 2021. Accessed March 10, 2022. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-10-20-21/08-COVID-Klein-508.pdf
6.
Montgomery J, Ryan M, Engler R, et al. Myocarditis following immunization with mRNA COVID-19 vaccines in members of the US military. JAMA Cardiol. 2021;6(10):1202-1206. doi:10.1001/jamacardio.2021.2833
ArticlePubMedGoogle ScholarCrossref
7.
Centers for Disease Control and Prevention Advisory Committee on Immunization Practices meeting. Myopericarditis following COVID-19 vaccination: updates from the Vaccine Adverse Event Reporting System (VAERS). October 21, 2021. Accessed March 10, 2022. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-10-20-21/07-COVID-Su-508.pdf
8.
US Food and Drug Administration Vaccines and Related Biological Products Advisory Committee Meeting. Surveillance updates of myocarditis/pericarditis and mRNA COVID-19 vaccination in the FDA BEST System. October 14, 2021. Accessed March 10, 2022. https://www.fda.gov/media/153090/download
9.
Centers for Disease Control and Prevention Advisory Committee on Immunization Practices meeting. COVID-19 vaccine safety updates. October 21, 2021. Accessed March 10, 2022. https://www.cdc.gov/vaccines/acip/m...es-2021-10-20-21/06-COVID-Shimabukuro-508.pdf
10.
Government of Ontario. Canada. Ontario recommends the use of Pfizer-BioNTech COVID-19 vaccine for individuals aged 18-24 years old. Published online September 29, 2021. Accessed September 29, 2021. Ontario Newsroom
11.
EPI-PHARE. Myocardite et péricardite après la vaccination Covid-19 [in French]. Published online November 8, 2021. Accessed November 9, 2021. Myocardite et péricardite après la vaccination Covid-19
12.
Ljung R, Sundström A, Grünewald M, et al. The profile of the Covid-19 vaccination register safety study in Sweden (CoVacSafe-SE). Ups J Med Sci. 2021;126. doi:10.48101/ujms.v126.8136 PubMedGoogle Scholar
13.
Laugesen K, Ludvigsson JF, Schmidt M, et al. Nordic Health Registry–based research: a review of health care systems and key registries. Clin Epidemiol. 2021;13:533-554. doi:10.2147/CLEP.S314959 PubMedGoogle ScholarCrossref
14.
Ludvigsson JF, Håberg SE, Knudsen GP, et al. Ethical aspects of registry-based research in the Nordic countries. Clin Epidemiol. 2015;7:491-508. doi:10.2147/CLEP.S90589 PubMedGoogle Scholar
15.
Schultz NH, Sørvoll IH, Michelsen AE, et al. Thrombosis and thrombocytopenia after ChAdOx1 nCoV-19 vaccination. N Engl J Med. 2021;384(22):2124-2130. doi:10.1056/NEJMoa2104882 PubMedGoogle ScholarCrossref
16.
Pottegård A, Lund LC, Karlstad Ø, et al. Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population based cohort study. BMJ. 2021;373(1114):n1114. doi:10.1136/bmj.n1114 PubMedGoogle Scholar
17.
Sera F, Armstrong B, Blangiardo M, Gasparrini A. An extended mixed-effects framework for meta-analysis. Stat Med. 2019;38(29):5429-5444. doi:10.1002/sim.8362 PubMedGoogle ScholarCrossref
18.
R Core Team. The R Project for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria; 2021. Accessed November 9, 2021. https://www.r-project.org
19.
Cochran WG. The comparison of percentages in matched samples. Biometrika. 1950;37(3-4):256-266. doi:10.1093/biomet/37.3-4.256 PubMedGoogle ScholarCrossref
20.
US Food and Drug Administration. Spikevax. February 18, 2022. Accessed February 21, 2022. SPIKEVAX
21.
US Food and Drug Administration. Comirnaty (previously COVID-19 vaccine Moderna). December 16, 2021. Accessed February 21, 2022. (COVID-19 Vaccine, mRNA)
22.
European Medicines Agency. Spikevax (previously COVID-19 vaccine Moderna). February 21, 2022. Accessed February 12, 2022. Spikevax (previously COVID-19 Vaccine Moderna) - European Medicines Agency
23.
European Medicines Agency (EMA). Comirnaty. February 16, 2022. Accessed February 21, 2022. Comirnaty - European Medicines Agency
24.
American College of Cardiology. Perspectives: vaccine-associated myocarditis risk in context: emerging evidence. February 9, 2022. Accessed February 21, 2022. Vaccine-Associated Myocarditis Risk in Context: Emerging Evidence - American College of Cardiology
25.
World Health Organization. WHO coronavirus (COVID-19) dashboard. Accessed February 16, 2022. https://covid19.who.int
26.
Andrews N, Stowe J, Kirsebom F, et al. Covid-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N Engl J Med. 2022. Published online March 2, 2022. doi:10.1056/NEJMoa2119451PubMedGoogle Scholar
27.
Bager P, Wohlfahrt J, Bhatt S, et al. Reduced risk of hospitalisation associated with infection with SARS-CoV-2 Omicron relative to Delta: a Danish cohort study. Lancet. Published online January 14, 2022. doi:10.2139/ssrn.4008930Google Scholar
28.
Lyngse FP, Kirkeby CT, Denwood M, et al. Transmission of SARS-CoV-2 Omicron VOC subvariants BA.1 and BA.2: evidence from Danish households. medRxiv. Preprint posted online January 30, 2022. doi:10.1101/2022.01.28.22270044Google Scholar
29.
Ioannou GN, Locke ER, Green PK, Berry K. Comparison of Moderna versus Pfizer-BioNTech COVID-19 vaccine outcomes: a target trial emulation study in the U.S. Veterans Affairs healthcare system. EClinicalMedicine. 2022;45:101326. doi:10.1016/j.eclinm.2022.101326PubMedGoogle Scholar
30.
Dickerman BA, Gerlovin H, Madenci AL, et al. Comparative effectiveness of BNT162b2 and mRNA-1273 vaccines in US veterans. N Engl J Med. 2022;386(2):105-115. doi:10.1056/NEJMoa2115463 PubMedGoogle ScholarCrossref
31.
Dagan N, Barda N, Balicer RD. Adverse effects after BNT162b2 vaccine and SARS-CoV-2 infection, according to age and sex. N Engl J Med. 2021;385(24):2299. doi:10.1056/NEJMc2115045PubMedGoogle ScholarCrossref
32.
Barda N, Dagan N, Ben-Shlomo Y, et al. Safety of the BNT162b2 mRNA Covid-19 vaccine in a nationwide setting. N Engl J Med. 2021;385(12):1078-1090. doi:10.1056/NEJMoa2110475 PubMedGoogle ScholarCrossref
33.
Patone M, Mei XW, Handunnetthi L, et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat Med. 2022;28(2):410-422. doi:10.1038/s41591-021-01630-0PubMedGoogle ScholarCrossref
34.
Husby A, Hansen JV, Fosbøl E, et al. SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study. BMJ. 2021;375:e068665. doi:10.1136/bmj-2021-068665 PubMedGoogle Scholar
the term often forwarded is 'monoclonal antibodies' ....
Monoclonal antibody - Wikipedia
en.wikipedia.org
this is the dif betwixt 'vaccine' and 'therapy'
~S~
Never met someone on the forum who is as wrong as you.
And you profess to be an expert. lol
That isn't true in my state or any of the states or areas I'm familiar with. Currently being compiled data shows the exact opposite of this.

 www.9news.com
www.9news.com
you obviously have no idea what these studies state... Bravo..1.
European Medicines Agency (EMA). COVID-19 mRNA vaccines Comirnaty and Spikevax: risk of myocarditis pericarditis. Published online July 19, 2021. Accessed November 9, 2021. COVID-19 mRNA Vaccines Comirnaty and Spikevax: risk of myocarditis pericarditis - European Medicines Agency
2.
Mevorach D, Anis E, Cedar N, et al. Myocarditis after BNT162b2 mRNA vaccine against Covid-19 in Israel. N Engl J Med. Published online October 6, 2021. doi:10.1056/NEJMoa2109730
3.
Witberg G, Barda N, Hoss S, et al. Myocarditis after Covid-19 vaccination in a large health care organization. N Engl J Med. Published online October 6, 2021. doi:10.1056/NEJMoa2110737
4.
Klein NP, Lewis N, Goddard K, et al. Surveillance for adverse events after COVID-19 mRNA vaccination. JAMA. 2021;326(14):1390-1399. doi:10.1001/jama.2021.15072
ArticlePubMedGoogle ScholarCrossref
5.
Centers for Disease Control and Prevention Advisory Committee on Immunization Practices meeting. Myocarditis analyses in the vaccine safety datalink: rapid cycle analyses and “head-to-head” product comparisons. October 21, 2021. Accessed March 10, 2022. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-10-20-21/08-COVID-Klein-508.pdf
6.
Montgomery J, Ryan M, Engler R, et al. Myocarditis following immunization with mRNA COVID-19 vaccines in members of the US military. JAMA Cardiol. 2021;6(10):1202-1206. doi:10.1001/jamacardio.2021.2833
ArticlePubMedGoogle ScholarCrossref
7.
Centers for Disease Control and Prevention Advisory Committee on Immunization Practices meeting. Myopericarditis following COVID-19 vaccination: updates from the Vaccine Adverse Event Reporting System (VAERS). October 21, 2021. Accessed March 10, 2022. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-10-20-21/07-COVID-Su-508.pdf
8.
US Food and Drug Administration Vaccines and Related Biological Products Advisory Committee Meeting. Surveillance updates of myocarditis/pericarditis and mRNA COVID-19 vaccination in the FDA BEST System. October 14, 2021. Accessed March 10, 2022. https://www.fda.gov/media/153090/download
9.
Centers for Disease Control and Prevention Advisory Committee on Immunization Practices meeting. COVID-19 vaccine safety updates. October 21, 2021. Accessed March 10, 2022. https://www.cdc.gov/vaccines/acip/m...es-2021-10-20-21/06-COVID-Shimabukuro-508.pdf
10.
Government of Ontario. Canada. Ontario recommends the use of Pfizer-BioNTech COVID-19 vaccine for individuals aged 18-24 years old. Published online September 29, 2021. Accessed September 29, 2021. Ontario Newsroom
11.
EPI-PHARE. Myocardite et péricardite après la vaccination Covid-19 [in French]. Published online November 8, 2021. Accessed November 9, 2021. Myocardite et péricardite après la vaccination Covid-19
12.
Ljung R, Sundström A, Grünewald M, et al. The profile of the Covid-19 vaccination register safety study in Sweden (CoVacSafe-SE). Ups J Med Sci. 2021;126. doi:10.48101/ujms.v126.8136 PubMedGoogle Scholar
13.
Laugesen K, Ludvigsson JF, Schmidt M, et al. Nordic Health Registry–based research: a review of health care systems and key registries. Clin Epidemiol. 2021;13:533-554. doi:10.2147/CLEP.S314959 PubMedGoogle ScholarCrossref
14.
Ludvigsson JF, Håberg SE, Knudsen GP, et al. Ethical aspects of registry-based research in the Nordic countries. Clin Epidemiol. 2015;7:491-508. doi:10.2147/CLEP.S90589 PubMedGoogle Scholar
15.
Schultz NH, Sørvoll IH, Michelsen AE, et al. Thrombosis and thrombocytopenia after ChAdOx1 nCoV-19 vaccination. N Engl J Med. 2021;384(22):2124-2130. doi:10.1056/NEJMoa2104882 PubMedGoogle ScholarCrossref
16.
Pottegård A, Lund LC, Karlstad Ø, et al. Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population based cohort study. BMJ. 2021;373(1114):n1114. doi:10.1136/bmj.n1114 PubMedGoogle Scholar
17.
Sera F, Armstrong B, Blangiardo M, Gasparrini A. An extended mixed-effects framework for meta-analysis. Stat Med. 2019;38(29):5429-5444. doi:10.1002/sim.8362 PubMedGoogle ScholarCrossref
18.
R Core Team. The R Project for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria; 2021. Accessed November 9, 2021. https://www.r-project.org
19.
Cochran WG. The comparison of percentages in matched samples. Biometrika. 1950;37(3-4):256-266. doi:10.1093/biomet/37.3-4.256 PubMedGoogle ScholarCrossref
20.
US Food and Drug Administration. Spikevax. February 18, 2022. Accessed February 21, 2022. SPIKEVAX
21.
US Food and Drug Administration. Comirnaty (previously COVID-19 vaccine Moderna). December 16, 2021. Accessed February 21, 2022. (COVID-19 Vaccine, mRNA)
22.
European Medicines Agency. Spikevax (previously COVID-19 vaccine Moderna). February 21, 2022. Accessed February 12, 2022. Spikevax (previously COVID-19 Vaccine Moderna) - European Medicines Agency
23.
European Medicines Agency (EMA). Comirnaty. February 16, 2022. Accessed February 21, 2022. Comirnaty - European Medicines Agency
24.
American College of Cardiology. Perspectives: vaccine-associated myocarditis risk in context: emerging evidence. February 9, 2022. Accessed February 21, 2022. Vaccine-Associated Myocarditis Risk in Context: Emerging Evidence - American College of Cardiology
25.
World Health Organization. WHO coronavirus (COVID-19) dashboard. Accessed February 16, 2022. https://covid19.who.int
26.
Andrews N, Stowe J, Kirsebom F, et al. Covid-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N Engl J Med. 2022. Published online March 2, 2022. doi:10.1056/NEJMoa2119451PubMedGoogle Scholar
27.
Bager P, Wohlfahrt J, Bhatt S, et al. Reduced risk of hospitalisation associated with infection with SARS-CoV-2 Omicron relative to Delta: a Danish cohort study. Lancet. Published online January 14, 2022. doi:10.2139/ssrn.4008930Google Scholar
28.
Lyngse FP, Kirkeby CT, Denwood M, et al. Transmission of SARS-CoV-2 Omicron VOC subvariants BA.1 and BA.2: evidence from Danish households. medRxiv. Preprint posted online January 30, 2022. doi:10.1101/2022.01.28.22270044Google Scholar
29.
Ioannou GN, Locke ER, Green PK, Berry K. Comparison of Moderna versus Pfizer-BioNTech COVID-19 vaccine outcomes: a target trial emulation study in the U.S. Veterans Affairs healthcare system. EClinicalMedicine. 2022;45:101326. doi:10.1016/j.eclinm.2022.101326PubMedGoogle Scholar
30.
Dickerman BA, Gerlovin H, Madenci AL, et al. Comparative effectiveness of BNT162b2 and mRNA-1273 vaccines in US veterans. N Engl J Med. 2022;386(2):105-115. doi:10.1056/NEJMoa2115463 PubMedGoogle ScholarCrossref
31.
Dagan N, Barda N, Balicer RD. Adverse effects after BNT162b2 vaccine and SARS-CoV-2 infection, according to age and sex. N Engl J Med. 2021;385(24):2299. doi:10.1056/NEJMc2115045PubMedGoogle ScholarCrossref
32.
Barda N, Dagan N, Ben-Shlomo Y, et al. Safety of the BNT162b2 mRNA Covid-19 vaccine in a nationwide setting. N Engl J Med. 2021;385(12):1078-1090. doi:10.1056/NEJMoa2110475 PubMedGoogle ScholarCrossref
33.
Patone M, Mei XW, Handunnetthi L, et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat Med. 2022;28(2):410-422. doi:10.1038/s41591-021-01630-0PubMedGoogle ScholarCrossref
34.
Husby A, Hansen JV, Fosbøl E, et al. SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study. BMJ. 2021;375:e068665. doi:10.1136/bmj-2021-068665 PubMedGoogle Scholar
the term often forwarded is 'monoclonal antibodies' ....
Monoclonal antibody - Wikipedia
this is the dif betwixt 'vaccine' and 'therapy'
~S~
How much faster? What age group are you talking about? What were their comorbidities?Vaccinated people cleared the virus faster,
you don't have a f-ing clue. Now those who were vaccinated are becoming the ones who die. Your vaccine was a short-term benefit and now the tables are turning because it did not allow the body's own immune system to function as it should.. Bravo... Moron..The covid vaccines were and are a triumph of science and have helped us get through a pandemic of a nasty, novel virus. As the virus burns through our population, fewer have been hospitalized or have died because of the vaccines. Vaccinated people cleared the virus faster, resulting in slower community transmission rates and less impact on our society and economy. The anti vaxx dummies did their best to sabotage it. But even through periods where 90% of hospitalized people were unvaccinated, we were vaccinated enough on the whole to prevent our healthcare infrastructure from collapsing.
Vaccines won, anti vaxx morons failed.
The covid vaccines were and are a triumph of science and have helped us get through a pandemic of a nasty, novel virus. As the virus burns through our population, fewer have been hospitalized or have died because of the vaccines. Vaccinated people cleared the virus faster, resulting in slower community transmission rates and less impact on our society and economy. The anti vaxx dummies did their best to sabotage it. But even through periods where 90% of hospitalized people were unvaccinated, we were vaccinated enough on the whole to prevent our healthcare infrastructure from collapsing.
Vaccines won, anti vaxx morons failed.
They are finding long term heart damage in people as old as 40 years of age... There was no reason to vaccinate these people but they forced it on them.. what these idiots did is criminal.You are totally wrong.
Since vaccination rates are over 70%, if the vaccines worked, the epidemic would have been long over. There simply are not enough unvaxed people left.
And now, the majority of those being infected and hospitalized ARE the vaxxed.
The number of vaccinated vs. unvaccinated patients in Colorado hospitals is changing
Before drawing any conclusions, the data needs context.
{...
The number of vaccinated vs. unvaccinated patients in Colorado hospitals is changing
DENVER — The number of vaccinated versus unvaccinated patients in Colorado hospitals is changing. But before drawing any conclusions, the data needs context.
Wednesday, the COVID data dashboard published by the Colorado Department of Public Health and Environment (CDPHE) showed 42 vaccinated hospitalized patients and 46 unvaccinated patients -- a near even split.
Thursday, the vaccinated outnumbered the other side with 59 patients compared to 44 unvaccinated patients.
For clarity, we spoke with Dr. Jon Samet with the Colorado School of Public Health, Dr. Reggie Washington, the chief medical officer with Presbyterian St. Luke's Medical Center, and CDPHE.
There are a few reasons these experts aren't surprised by the numbers.
"It's what we would expect, particularly with [the omicron COVID variant], many people who were unvaccinated became infected and now have natural acquired immunity," Samet said. "So, the pool of people unvaccinated is now increasingly immune because the omicron infection or delta [variant] before that. We see that change in proportion and would expect that."
CDPHE elaborated on that via email, saying that vaccine rates alone won't reflect other factors, especially when case counts are comparatively low.
"First, nearly 80% of Colorado's adult population and nearly 90% of the 65+ population is fully vaccinated. The "even split" is coming from very different sized populations. Additionally, older individuals are more likely to be vaccinated but are also more likely to be hospitalized.
At times of very low case counts, it is not unusual to see things like this 'even split,' or even potentially times when there may be more vaccinated people hospitalized than unvaccinated people."
All of that considered, by looking at sheer numbers, there can be more vaccinated patients because the vaccinated population is simply a much bigger group of people than those without the vaccine. When you break it down by age, a more apples-to-apple comparison, people without their shots end up in the hospital at a higher rate, CDPHE said.
...}
Correct.Wrong.
The mRNA provided a short 6 month increase in B-cell antibody production, but it did nothing at all for long term memory in T-cells. The mRNA vaccine was a total failure because it prevented herd immunity, so kept the epidemic going, essentially forever.
And now that the majority are vaccinated, the majority getting infected and being hospitalized are vaccinated.
The reality is that the correct procedure is to end any epidemic as quickly as possible.
The 2 methods are either full quarantine or herd immunity.
We did neither.
So instead we conserved easy hosts, so that it would never run out.
Oddly, tony kept begging us early on to get the experimental injection so that we can achieve herd immunity. He either knew that the experimental injection didn't confer immunity and decided to lie to us about that, or he didn't know that the experimental injection does not confer immunity, which would make him ignorant of the facts.The mRNA vaccine was a total failure because it prevented herd immunity,
He is wrong. Those who are vaccinate have a 10 times greater risk of becoming infected in the first 14 days. There after they have about a 3 times greater infection rate. The mRNA vaccines are not helpful in this area and were part of the reason for our spike in infections. They allowed asymptomatic spread. Masking did next to nothing and wasn't much more than a placebo to make people feel good. Not much of what the CDC or Fauci did was based in science.How much faster? What age group are you talking about? What were their comorbidities?
It was a monetary decision. As I understand it, Fauci is on the take from Big Pharma.. he didn't care what damage it did as long as his pockets got fat with money.Oddly, tony kept begging us early on to get the experimental injection so that we can achieve herd immunity. He either knew that the experimental injection didn't confer immunity and decided to lie to us about that, or he didn't know that the experimental injection does not confer immunity, which would make him ignorant of the facts.
Those are the two choices. Did he lie? Or was he ignorant?
And this is the key.... Biden was set to keep the shots coming forever. Making us dependent on the government for our very lives and lining the pockets of those who donated to his campaign. Corrupt bastards to the very core. This is why they wanted no one to look into natural immunities and why they are so superior to the man made crap.The mRNA vaccine was a total failure because it prevented herd immunity, so kept the epidemic going, essentially forever.
Unfortunately, a lot of humans have not evolved to the extent necessary to avoid exploitation by humanity's sellouts. Instead of seeing them for what they are, they revere them out of a conditioned loyalty to authority.It was a monetary decision. As I understand it, Fauci is on the take from Big Pharma.. he didn't care what damage it did as long as his pockets got fat with money.