Greenbeard
Gold Member
Health economist/professor/NYT contributor Uwe Reinhardt wrote a brief article on the Economix blog the other day presenting some of the ideas he put forth in a paper, "The Many Different Prices Paid To Providers And The Flawed Theory Of Cost Shifting: Is It Time For A More Rational All-Payer System?", in this month's Health Affairs (the full text of which is apparently free until Wednesday).
The subject Reinhardt focuses on is the sometimes vast differences different payers pay for the same health services:
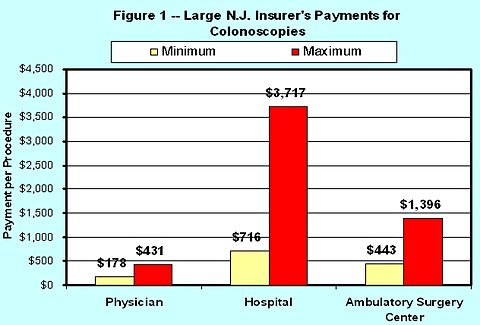
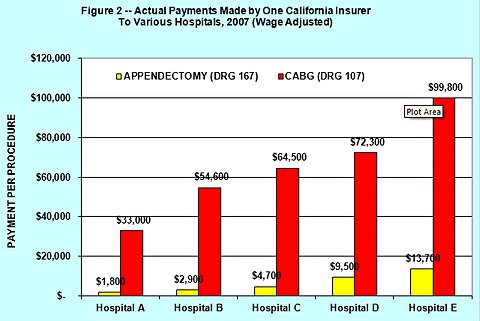
While that variation occurs within a given facility, he throws in some graphics from the insurer's perspective (seeing huge variations for a given service between facilities):
Ultimately, as its title suggests, Reinhardt's paper is about proposing an all-payer system:
Food for thought.
The subject Reinhardt focuses on is the sometimes vast differences different payers pay for the same health services:
My paper focuses on the fact that every private health insurer in this country pays different physicians, hospitals and other providers of health care different prices for identical services. The flip side of this practice is that a given provider charges different payers insurers or patients different prices for identical health service. Economists call that practice price discrimination.
While that variation occurs within a given facility, he throws in some graphics from the insurer's perspective (seeing huge variations for a given service between facilities):
Ultimately, as its title suggests, Reinhardt's paper is about proposing an all-payer system:
Other nations with multiple insurance carriers for example, Germany and Switzerland avoid price discrimination in health care through negotiations over prices between regional associations of health insurers and counterpart associations of health care providers, subject to some overall budget constraint informed by macroeconomic conditions (e.g., growth of the payroll on which premiums are based or per capita income). The negotiated prices then apply uniformly to all insurers and all providers in a region (states in Germany and cantons in Switzerland). In the United States, Maryland has operated such an all payer system for hospitals for several decades.
An all payer system has the potential to reduce health care costs in several ways, including the discipline of a fee schedule on providers, the schedule to be negotiated with providers on a regional basis, and a reduction in the enormous complexity and high administrative costs of the current system.
If it is desired, an all payer system can also serve as a way to constrain the future growth of health care to some desired path e.g., with total national health spending growing annually only 0.5 percentage points faster than the growth of the rest of gross the domestic product, rather than the traditional two percentage points faster that prevailed over the last four decades. A two percentage point differential is simply not sustainable.
In my above-cited paper, I advocate an all payer system for the United States to eliminate the pervasive price discrimination inherent in American health care and, to the extent it exists, the much-lamented cost shift. For readers of this blog, Health Affairs has graciously provided access to the paper until Nov. 16. I invite readers to take a look at my argument for an all-payer approach and share with us their reaction to it.
Food for thought.