Sun Devil 92
Diamond Member
- Apr 2, 2015
- 32,078
- 11,094
- 1,410
- Banned
- #1
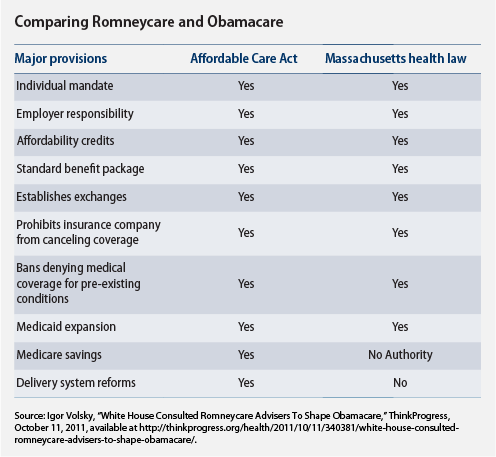
Romneycare Improved Health Outcomes, Thanks To Private-Sector Coverage
The article shows that having insurance improves outcomes. Private insurance.
**********************************************************************
As you may know if you’re a regular reader of The Apothecary, the left has systematically ignored the mountains of clinical evidence showing that the Medicaid program doesn’t actually make people healthier. Given that Obamacare is designed to achieve half of its coverage expansion via Medicaid, you can understand why: if Medicaid doesn’t make people healthier, a significant chunk of Obamacare is wasted money. But the other chunk of Obamacare—the one that expands coverage using subsidized private-sector coverage—could indeed have an impact on health outcomes. An important new study, following the health outcomes of Romneycare in Massachusetts, shows us how.
^^^^^^^^^^
The usual Obamacare cheerleaders on the left are arguing that the AIM study is one more reason to expand Medicaid. But the opposite is true. The study gives us no evidence that Medicaid improved health outcomes, because Romneycare expanded coverage primarily through private insurance.
And it turns out that the number of people with private coverage actually goes up if you don’t expand Medicaid in your state.
There are two reasons for this. The first is that eligibility for Obamacare’s exchanges expands if you don’t expand Medicaid. In states that do expand Medicaid, exchange subsidies are available for people whose incomes are between 138 and 400 percent of the federal poverty level. In states that don’t expand Medicaid, people with incomes between 100-138 percent of FPL also become eligible for the exchanges.
In addition, a good chunk of those who are uninsured and would qualify for Medicaid under an expansion already have access to coverage through their employers. For example, a study of Medicaid expansion in New Hampshire by the Lewin Group found that, of the state population eligible for the Medicaid expansion, three-fifths would gain private coverage through either their employers or the exchanges if the state didn’t expand Medicaid.
The article shows that having insurance improves outcomes. Private insurance.
**********************************************************************
As you may know if you’re a regular reader of The Apothecary, the left has systematically ignored the mountains of clinical evidence showing that the Medicaid program doesn’t actually make people healthier. Given that Obamacare is designed to achieve half of its coverage expansion via Medicaid, you can understand why: if Medicaid doesn’t make people healthier, a significant chunk of Obamacare is wasted money. But the other chunk of Obamacare—the one that expands coverage using subsidized private-sector coverage—could indeed have an impact on health outcomes. An important new study, following the health outcomes of Romneycare in Massachusetts, shows us how.
^^^^^^^^^^
The usual Obamacare cheerleaders on the left are arguing that the AIM study is one more reason to expand Medicaid. But the opposite is true. The study gives us no evidence that Medicaid improved health outcomes, because Romneycare expanded coverage primarily through private insurance.
And it turns out that the number of people with private coverage actually goes up if you don’t expand Medicaid in your state.
There are two reasons for this. The first is that eligibility for Obamacare’s exchanges expands if you don’t expand Medicaid. In states that do expand Medicaid, exchange subsidies are available for people whose incomes are between 138 and 400 percent of the federal poverty level. In states that don’t expand Medicaid, people with incomes between 100-138 percent of FPL also become eligible for the exchanges.
In addition, a good chunk of those who are uninsured and would qualify for Medicaid under an expansion already have access to coverage through their employers. For example, a study of Medicaid expansion in New Hampshire by the Lewin Group found that, of the state population eligible for the Medicaid expansion, three-fifths would gain private coverage through either their employers or the exchanges if the state didn’t expand Medicaid.