- Thread starter
- #81
Progress against malaria could be lost to funding cuts...

Malaria Programs at Risk From Funding Cuts
December 21, 2012 - World Health Organization also warns in its annual report that latest drugs could soon become ineffective against some deadly malarial parasites
Malaria Programs at Risk From Funding Cuts
December 21, 2012 - World Health Organization also warns in its annual report that latest drugs could soon become ineffective against some deadly malarial parasites
Funding for programs to control malaria and provide universal treatment for the mosquito-borne disease is falling short of international goals, according to the World Health Organization. In its annual report, the WHO also warns that the latest drugs could soon become ineffective against some deadly malarial parasites. Ami Diabate, has brought her three children to a rural clinic to get the latest anti-malarial drugs. The aid agency Médecins Sans Frontières - or Doctors Without Borders - is rolling out the pilot program across Mali. Results are encouraging - a 65-percent drop in infections a week after distribution.
Deadly disease
Diabate said she has noticed an immediate difference. "My children used to have fevers regularly, she said, but since they started taking this medicine, they haven't run a temperature." Malaria kills an estimated 660,000 people every year. Over the past decade, advances in prevention and treatment have cut the death rate by 30 percent. The World Health Organization warns, however, that funding increases over the past two years have slowed significantly - putting such progress at risk. Simon Wright is head of child survival at the aid agency, Save the Children. The financial crisis means that a lot of governments - not all by any means - but a lot of governments are tailing off in their aid budgets. And so where we were seeing growth were not seeing growth any more. But also theres a factor of maybe donors changing their interests, said Wright.
Short on supplies
In 2011, international donors made $2.3 billion available to fight malaria - less than half the $5.1 billion that the WHO says is needed annually. The money goes toward some simple tools, said Professor Sir Brian Greenwood of the London School of Hygiene and Tropical Medicine. One of those is the humble bed-net, which people have been using for hundreds of years. But the relatively new advance has been in treating the nets with insecticide. Now, the insecticide is actually incorporated into the material, he said. The number of insecticide-impregnated nets delivered to sub-Saharan Africa fell from 145 million in 2010 to 66 million in 2012. Indoor spraying programs also have leveled off.
Increased resistance
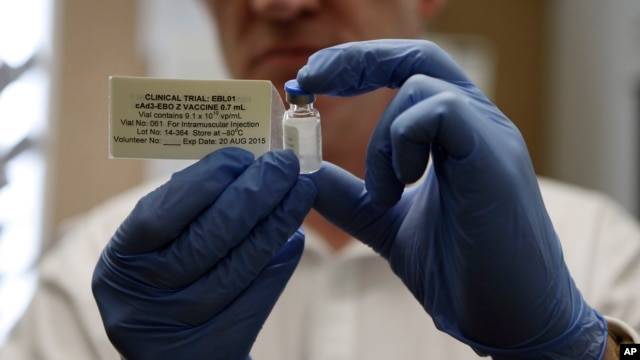
Greenwood said the greatest concern is the growing resistance of the malarial parasite to the latest medicines known as artemisinins. We do have now quite clear evidence that there is resistance to the artemisinins, particularly in Cambodia, but probably in the neighboring countries. Fortunately not yet in Africa, but it would be a disaster if those parasites got loose in Africa, and our main treatment was failing again, like it did with chloroquin, he said. Until an effective malaria vaccine is developed and made available globally, researchers say it is vital that donors continue to fund prevention and treatment programs that have made such progress until now.
Source